Semaglutide vs. Tirzepatide vs. Retatrutide: Which GLP-1 Is Right for You?
By Bryce Johnson ·

If you've started researching medical weight loss, you've probably run into three names — semaglutide, tirzepatide, and retatrutide — and wondered how they actually differ. Whether you're searching semaglutide vs tirzepatide or tirzepatide vs semaglutide, both medications are FDA-approved and widely prescribed, while retatrutide is generating buzz even though it isn't approved yet. Below, we break down how each medication works, the trial data, honest side effects, and how our nurse practitioners decide which option — if any — fits a given patient.
Quick Answer: Semaglutide vs. Tirzepatide vs. Retatrutide at a Glance
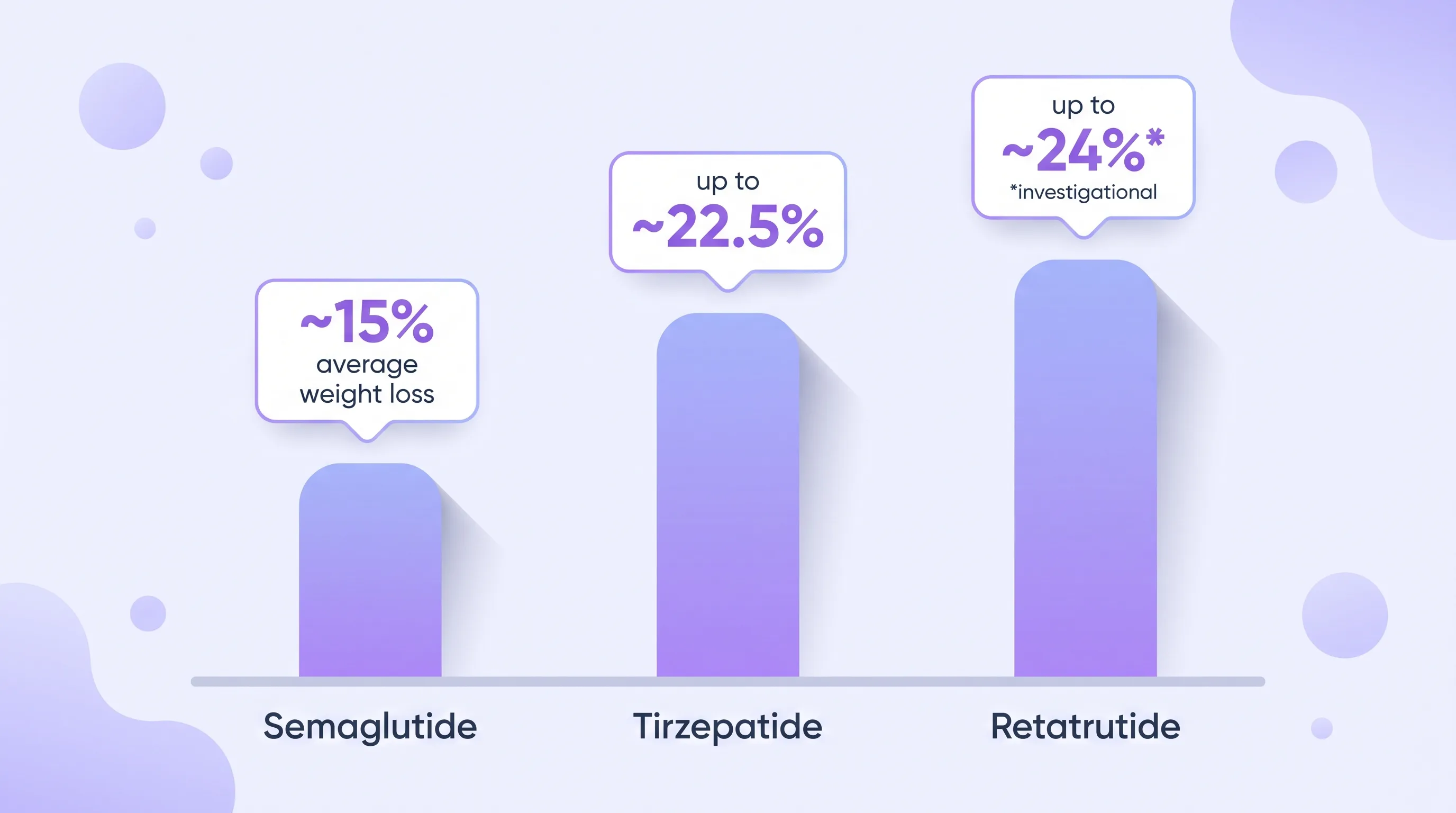
In short: semaglutide and tirzepatide are both FDA-approved GLP-1 medications with strong safety records, while retatrutide is still investigational and not something you can currently be prescribed. Tirzepatide's trial data shows somewhat greater average weight loss than semaglutide's, and retatrutide's early data is higher still — but "more weight lost in a trial" doesn't automatically mean it's the right choice for you.
| Drug | Mechanism | FDA Status | Avg. Weight Loss (trial) | Common Side Effects |
|---|---|---|---|---|
| Semaglutide (Ozempic/Wegovy) | GLP-1 receptor agonist | FDA-approved (Ozempic, type 2 diabetes, 2017; Wegovy, chronic weight management, 2021) | ~14.9% at 68 weeks vs. 2.4% placebo | Nausea, vomiting, diarrhea, constipation, abdominal pain |
| Tirzepatide (Mounjaro/Zepbound) | Dual GLP-1/GIP agonist | FDA-approved (Mounjaro, type 2 diabetes, May 2022; Zepbound, chronic weight management, Nov. 2023) | 16.0–22.5% at 72 weeks (dose-dependent) vs. 2.4% placebo | Similar GI profile to semaglutide, slightly higher at top doses |
| Retatrutide | Triple GLP-1/GIP/glucagon agonist | Investigational — not FDA-approved for any use as of 2026; Phase 3 trials ongoing | ~17.5% at 24 weeks, ~24.2% at 48 weeks (Phase 2) vs. ~2.1% placebo | Similar GI effects; early trials noted transient increases in heart rate |
We'll unpack each of these medications individually below, including what the numbers mean in practice and what tends to make someone a better fit for one over another.
How GLP-1 Medications Work for Weight Loss
GLP-1 medications work by mimicking incretin hormones — natural signals your gut releases after eating that tell your brain and pancreas how to respond. In plain English, they slow digestion, help you feel full sooner and longer, and improve how your body manages blood sugar — together reducing overall calorie intake.
GLP-1 (glucagon-like peptide-1) is one of several incretin hormones your body already makes. Semaglutide targets the GLP-1 receptor alone, while tirzepatide and retatrutide also engage additional receptors — GIP, and in retatrutide's case, glucagon too — which is part of why trial results differ between them. Choosing a GLP-1 for weight loss ultimately comes down to matching that mechanism, and its side-effect profile, to your health history. We cover this in more depth, along with other peptides sometimes discussed for weight loss, in our guide to peptides for weight loss.
Semaglutide (Ozempic/Wegovy): The FDA-Approved GLP-1 Standard
Semaglutide is the original mainstream GLP-1 for weight loss, approved by the FDA as Ozempic for type 2 diabetes in 2017 and as Wegovy for chronic weight management in 2021. It also has the longest real-world track record of the three, with years of post-approval prescribing experience.
In the STEP 1 trial published in the New England Journal of Medicine, participants taking semaglutide lost an average of about 14.9% of their body weight over 68 weeks, compared to 2.4% in the placebo group, and 86.4% of participants achieved at least 5% weight loss. For many patients, semaglutide is a reasonable starting point, particularly those newer to GLP-1 therapy or with a preference for the medication with the longest history of use. Semaglutide therapy is typically delivered as part of a broader clinician-guided medical weight loss program that includes lab monitoring, dose titration, and nutrition support rather than as a standalone prescription.
Tirzepatide (Mounjaro/Zepbound): The Dual GLP-1/GIP Agonist
Tirzepatide is a newer GLP-1 medication that also activates the GIP receptor, and its trial data shows somewhat greater average weight loss than semaglutide's at comparable trial lengths. It was FDA-approved as Mounjaro for type 2 diabetes in May 2022 and as Zepbound for chronic weight management in November 2023.
The SURMOUNT-1 trial, also published in the New England Journal of Medicine, found that participants lost an average of 16.0% of body weight at the 5mg dose, 21.4% at 10mg, and 22.5% at the highest 15mg dose over 72 weeks, compared to 2.4% in the placebo group — with 89% to 96% of participants (depending on dose) reaching at least 5% weight loss. Because tirzepatide engages two receptor pathways instead of one, some patients who plateau on semaglutide see additional progress after switching, though individual response always varies. This dose-dependent gap is the crux of most tirzepatide vs semaglutide conversations with our providers.
Retatrutide: The Investigational Triple Agonist
Retatrutide is a triple agonist that targets the GLP-1, GIP, and glucagon receptors, and it is currently investigational — not FDA-approved for any indication as of 2026. It's still moving through the Phase 3 TRIUMPH trial program, with an FDA decision not expected until roughly late 2027, so no clinic can legally prescribe it for weight loss today.
The Phase 2 data, published in the New England Journal of Medicine, showed participants losing an average of about 17.5% of body weight at 24 weeks and roughly 24.2% at 48 weeks, compared to about 2.1% in the placebo group — numbers that have understandably generated a lot of interest. Patients sometimes ask about retatrutide vs tirzepatide head-to-head, but that comparison is premature until Phase 3 results are in and FDA review is complete. Early trials also noted transient increases in heart rate, and long-term safety data is still accruing. Compounded versions of retatrutide sometimes advertised online exist in a legally murky gray area outside FDA oversight, and we don't recommend or prescribe them; the responsible path is to wait for FDA review of the completed trial data.
Semaglutide vs. Tirzepatide Side Effects: What's Common Across All Three
All three GLP-1 medications share a similar side-effect profile, dominated by gastrointestinal symptoms — nausea, vomiting, diarrhea, constipation, and abdominal pain — that are dose-dependent and most noticeable during dose increases. Research published in Mayo Clinic Proceedings in 2025 estimates GI effects affect roughly 40% to 70% of patients on GLP-1 therapy, though symptoms typically ease as dosing stabilizes.
One honest consideration across semaglutide, tirzepatide, and retatrutide alike: significant weight loss can include some loss of lean muscle mass alongside fat, which is why ongoing monitoring matters, not just the number on the scale. Tracking body composition with tools like our InBody scales can help distinguish fat loss from muscle loss, so adjustments to protein intake or activity level can be made if needed.
Who Tends to Do Best With Each Option
There's no single answer to the semaglutide vs tirzepatide for weight loss question — the right choice depends on your health history, prior treatment response, GI tolerance, and goals more than trial averages alone. Someone newer to GLP-1 therapy often does well starting with semaglutide. Someone who has plateaued on semaglutide, or who has type 2 diabetes alongside a weight goal, may be a better candidate for tirzepatide given its dual mechanism. And anyone drawn to retatrutide should understand that, as of 2026, it simply isn't available outside clinical trials.
If you're not sure where your hormones and metabolism stand before considering any GLP-1 option, our hormone assessment quiz is a useful starting point before your first visit.
Cost, Insurance & the Compounding Reality
Brand-name semaglutide (Wegovy) and tirzepatide (Zepbound) can be expensive without insurance, and coverage for weight-loss indications varies widely — some plans require prior authorization, many don't cover it at all, and rules change frequently. We can't promise specific pricing or guarantee coverage, since that depends entirely on your individual insurance plan and pharmacy. In practice, cost often becomes the deciding factor once the semaglutide vs tirzepatide for weight loss question has already been settled with your provider.
You may also encounter compounded semaglutide or tirzepatide, sometimes offered as a lower-cost alternative during manufacturer shortages. Compounded medications should only come from a licensed pharmacy as part of a monitored plan — never an unregulated online seller. Retatrutide compounds carry added legal uncertainty since the drug itself hasn't cleared FDA review, and we're not able to prescribe or recommend them.
How Care Works at Hormones + Weight Loss
At our clinics in Meridian, Twin Falls, and Lewiston, Idaho, GLP-1 treatment starts with a full health history and lab work — not a medication handed over on request. Our nurse practitioners use that information, along with your goals and any prior GLP-1 experience, to build an individualized plan within our clinician-guided medical weight loss program — including which medication, if any, and how your dose is titrated.
From there, care includes regular follow-up visits to track progress, manage side effects, and adjust course as needed — not a set-it-and-forget-it prescription. If you're in or near Meridian, Twin Falls, or Lewiston, that conversation with a provider is the right next step before choosing a medication.
Frequently Asked Questions
Semaglutide vs. tirzepatide — which is better for weight loss?
Tirzepatide's clinical trial data shows somewhat greater average weight loss than semaglutide's — up to 22.5% versus 14.9% at comparable trial lengths — but "better" depends on your individual health history, tolerance, and response. Both are FDA-approved and effective; a provider evaluation is the best way to determine which fits your situation.
Is tirzepatide safer than semaglutide, or similar risks?
Semaglutide and tirzepatide have broadly similar safety profiles, both dominated by gastrointestinal side effects, though tirzepatide's GI effects can run slightly higher at its top dose. Neither is inherently "safer" in a blanket sense — both require monitoring and are prescribed based on individual health history.
What are the side effects of semaglutide vs. tirzepatide?
Both medications share nausea, vomiting, diarrhea, constipation, and abdominal pain as the most common side effects, especially during dose increases. These generally ease as the body adjusts and dosing stabilizes, though ongoing monitoring by a provider is part of responsible GLP-1 treatment.
Can you switch from semaglutide to tirzepatide?
Yes, switching between GLP-1 medications is common when a patient plateaus or isn't tolerating one option well, but it should always be guided by a provider who can adjust dosing and monitor the transition. Individual results vary, and a switch is never guaranteed to produce a specific outcome.
Is retatrutide available now, or still investigational?
Retatrutide is still investigational and not FDA-approved as of 2026 — it remains in Phase 3 trials, with a potential FDA decision not expected until around late 2027. It cannot currently be prescribed for weight loss, and any retatrutide vs tirzepatide comparison remains theoretical until that review is complete.
Next Steps
Semaglutide and tirzepatide are both FDA-approved, well-studied GLP-1 options, while retatrutide remains a promising but investigational medication still working through clinical trials. The right choice between them isn't about which trial had the highest average — it's about your health history, goals, and how your body responds under proper monitoring. Our nurse practitioners in Meridian, Twin Falls, and Lewiston, Idaho can walk you through the options in detail — Book a Consultation to get started.


